Thousands of bright-eyed and bushy-tailed students recently found out whether they had been accepted into Australian medical schools.
Thousands of bright-eyed and bushy-tailed students recently found out whether they had been accepted into Australian medical schools.
Selection is a highly competitive process, requiring an impressive combination of high secondary school results (ATAR/GPA), high results on various medical admissions tests (UMAT/GAMSAT), cogent personal statements and/or performance in multiple mini interviews.
Only the most successful students are selected.As selection interviewers for an Australian medical school, one of our scripted questions was “How have you helped disadvantaged people?” A memorable candidate began, “well, our family has a maid…”.
Other applicants told stories of well-intentioned overseas trips to help “poor people” in other countries. Strikingly, of the nearly 20 aspirants we interviewed, none told stories of socioeconomic disadvantage involving themselves, family or friends.Although we cannot say whether these students were selected, it is likely some of them were.
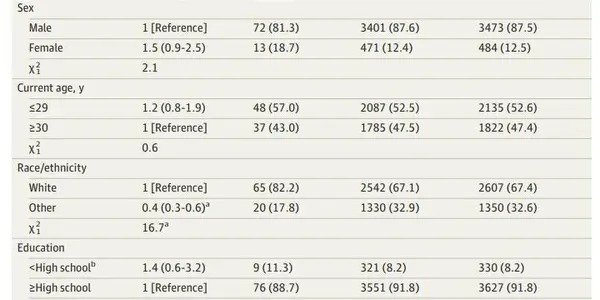
These well-to-do students will become the future of our medical system.About two-thirds of Australian medical students come from affluent backgrounds. Fewer than one in ten come from low socioeconomic status backgrounds.
This is unsurprising as selection criteria such as ATAR and personal statements are known to be biased against low-socioeconomic-status candidates.Universities have created special access schemes, and tests such as the Undergraduate Medical Admissions Test (UMAT), Graduate Australian Medical School Admissions Test (GAMSAT), personality tests and interviews which are supposed to reduce bias against low-socioeconomic-status candidates.
However, low-socioeconomic-status applicants are still less successful than their high-socioeconomic-status counterparts at getting into medical schools, perhaps due to the lack of access to role models, support, and opportunities necessary. Females from low socioeconomic backgrounds are the most disadvantaged.
Consequences for patients
Socioeconomic status is associated with important differences in values and beliefs.Two families recently delivered very premature newborn babies who needed life support. If the babies survived, they were faced with a high chance of disability requiring lifetime care.
The families came from different socioeconomic backgrounds, and expressed different concerns. The parents who were struggling with money said they would not be able to afford the high costs of looking after a disabled child.The well-off parents expressed they were worried the child’s disability was going to be so severe their child’s quality of life would not be worth putting the child through the intensive and traumatic treatments.
Although both sets of parents wished to withdraw care, they were perceived and treated differently by their health team. One set of parents was eventually referred to child protective services, and the other family had their wishes carried out.This example highlights the difficulties in shared decision-making when values and priorities are different, and the extent of their impact. People with lower socioeconomic status consistently have poorer health and are more likely to die earlier than their more affluent counterparts, and are less involved in medical decision-making.
Conversely, patients with higher socioeconomic status tend to be more assertive, take an active role in their medical management and receive more explanations.Selecting a medical community with such differences in socioeconomic status to the Australian population (in which only 25% of people are classified as affluent) holds the risk that the patients they serve have contrasting priorities, values and life situations to their own.
It is human nature to feel more comfortable with, and be more persuaded by patients who hold similar values and articulate them in a familiar way. Patients who have divergent preferences or goals of treatment may have their intentions misconstrued or experience conflict with their doctors.
What can be done?
Medical schools should continue refining medical selection processes to give students with lower socioeconomic status a fair opportunity to become doctors. The medical fraternity and patients would be better off with a broader representation of doctors from different backgrounds.
Doctors do not need to have the same backgrounds as their patients to deliver good care, but they should strive to understand and respect their patients’ needs, expectations and values when delivering health care. Doctors should be aware of the effects socioeconomic status has on the doctor-patient relationship and that patients’ intents and styles of communication may vary from their own.
Much emphasis has been placed on “cultural competency”, but this is often framed in racial, linguistic, ethnic and religious differences. The medical profession is more aware of the possibility of value conflicts when patients speak a different language or have a different ethnic, racial or religious background to their own.However, when a patient shares the same language or culture, there is an unsaid assumption that there will be common understandings. Expanding these lessons to socioeconomic status is essential to creating a system that serves those who need it most.![]()
By Evelyn Chan, Medical doctor (pediatrics and public health), Royal Children's Hospital and Paul Leong, Doctor, Monash Health. This article was originally published on The Conversation. Read the original article. Image credit: Shutterstock