One evening last spring, Peter nearly stopped breathing.
He was riding in the car with his mother, April, who was taking the 11-year-old boy back from a visit to the ER for one of his chronic asthma attacks. He seemed to be getting better — and then his throat began to constrict. He began to wheeze loudly. He rolled his head back to get more air.
"That was wrong. 'He should be better than this by now,' I remember thinking. I knew something was wrong then," April recalls. "They had given him some meds and the usual advice, but it was not working."
She turned the car around and drove her son back to the hospital, where physicians and technicians eventually stabilized Peter and, again, sent him home. "On the way home I realized what the doctors were saying," she remembers. "He had had a pneumothorax — a partially collapsed lung!"
At Hudson Elementary School in Long Beach, where Peter attends school, asthma is the big subject — in and out of the classroom. A hardscrabble cluster of buildings alongside the busy Terminal Island Freeway, Hudson is one of 20 sites targeted for intensive clinical intervention by UCLA asthma and immunology experts. With good reason: One out of five Hudson students — 20 percent — has asthma; the national average is 9.6 percent.
Worse, about 10 percent of those kids have uncontrolled asthma, meaning that the usual palette of inhalers, drugs, lifestyle and environmental changes simply doesn't work for them anymore. They can't breathe like normal kids. Many also have early signs of cardiovascular disease — heart arrhythmias and high cholesterol and sleep apnea.
Finding out why that is so — and how modern medicine might eventually find a cure — has long vexed the nation's public authorities and the scientists who stand behind them. Now it is the object of a tight-knit network of UCLA physicians, researchers and public-health experts. Not only are they trying to find the answer, they are also creating a new paradigm for air-quality control and treatment for the 21st century. That the problem stems not from factories and ozone, but from freeways and cars — the ultimate L.A. icons — makes their quest one of the more challenging in public health today.
An "Insult to the Immune System"
Intuitively, the tie between smog and respiratory disease seems obvious, but consensus over the whys and hows of that connection remains far from settled. Attempts to pin down the link have long been fraught with competing epidemiological data (many with competing political and regulatory agendas), poor understanding of the mechanisms underlying air pollution and lungs (good animal models for asthma are a recent innovation), and the seemingly impossible (until about 10 years ago) genetic connection: Why are some groups so vulnerable to emissions in the air and why are some seemingly protected?
That question has troubled Dr. Andre Nel, professor of medicine and chief of nanomedicine at the David Geffen School of Medicine at UCLA, since he came to Westwood some 24 years ago.
"When I got here, I was mainly interested in the science of the immune system, but with my lab on the 13th floor of the Jonsson Comprehensive Cancer Center, I was confronted every day with a view of the pollution haze over the city," Nel explains. "As a scientist, I began to wonder how that was affecting my clinical practice. So many of my patients had asthma and severe allergies; their immune systems were totally compromised. And I myself had flare-ups I never had before."
To find out what was driving the disease process, Nel and a number of his peers, along with colleagues at USC, first sought to define exactly what kind of air pollution was the problem. For years, the main indicator was ozone — the visible smog we can see on the horizon. But ozone turns out to be an imprecise measurement of disease risk. After all, the recent flare in asthma rates in particularly polluted L.A. neighborhoods came about while official air-pollution levels were still declining.
What was happening? Beginning in the '90s, researchers began to see: Not all smog was the same.
Nel's idea was to first simply describe the fundamentals. "The old way was to look at ozone levels," he says. "What you could see in the air. Now we are looking at the specific content of air in specific areas at specific times and measuring the size of the particles."
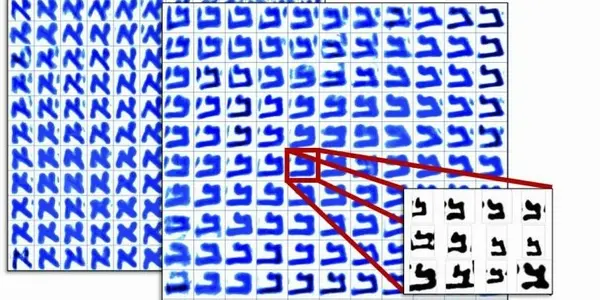
That led to one principal villain: ultrafine particles (UFPs) spewed out by cars and trucks. These carbon-filled "fresh emissions," as they are called, are so small (about 1/1000th of a human hair) that they can enter lung tissues and eventually spill over into the bloodstream, causing body-wide inflammation. Nel has managed to record a stunning visual image of a UFP's wreckage. He summons it up on his desktop computer screen. It is a photo of a cell; inside it one can seen the various sub-units — the nucleus, the cell membrane and such — and, right in the center, there is an ultrafine particle of road emission, stuck inside — and destroying — the mitochondria, the so-called energy plant of all life.
To understand the consequences of such cellular invasions, Nel and his associates exposed genetically susceptible lab mice to different kinds of particles and then compared them to mice breathing fresh air. The results were stunning: The mice getting the UFPs not only displayed a severely compromised immune system, but also possibly a decline in the effectiveness of high-density lipoprotein, or HDL, in their blood. "What we kept finding was that somehow, UFPs were making the good cholesterol less powerful in cleaning up bad cholesterol."
Since then, Nel's group has been teasing out the gene candidates that seem to drive this inflammatory process. Many relate to oxidative stress, the damage that occurs when UFPs generate free radicals, the volatile residuals of the cell's own energy-burning process.
When free radicals run rampant, it is only a matter of time before you get an immune system that overreacts to common environmental allergens, he says. "You get chronic lung inflammation, and your body's immune system can't fight disease."
Put that immune system in a modern city like Los Angeles, and you've got problems. As Dr. Marc Riedl M.S. '04, Nel's colleague in the Geffen School of Medicine, puts it: "The megacity of today is different from the megacity of the past. From the point of view of the lungs, the city is now an unprecedented insult to the immune system."
What (and Where) Is Up In the Air?
Looming over all of this is one still-unanswered question: Why are so many Los Angeles kids resistant to traditional asthma treatment, and why so many now, after so many years of vigorous air-quality control?
"It is all about GxE, or genes times environment, or environmental insults amplified by genetic predisposition," contends Dr. Maria Garcia-Lloret, assistant clinical professor of pediatric allergy and immunology at Mattel Children's Hospital UCLA and the founder of the UCLA Breathmobile, an RV-style, blue-and-gold mobile asthma clinic that rolls to school sites in Southern California like Peter's Hudson Elementary in Long Beach to give kids free diagnosis, treatment, medication and education.
The "E" of her "GxE" here is the freeway; at schools like Hudson, UFP levels are several times the average elsewhere in the region. And they are potent. UFPs are active — which means toxic — anywhere from 500-1,500 yards on each side of the freeway. In Hudson's case, the roaring Terminal Island Freeway, a central economic bloodline of modern Los Angeles.
All right, but what about the "G," the genes? How did they mutate in such a short period of time, and why would this generation carry it so widely? It is not a theoretical problem for Garcia-Lloret. She sees its consequences every day.
"You know, we went into these neighborhoods with this very straightforward public-health approach," she explains. "We thought these children were sick because they did not have access to care, to the right meds, etc., and that if we could give them that they would not be going to the ER so much anymore … [But] even with maximal treatment, these kids were still symptomatic." Severely, in cases like Peter's.
Solutions have been stubbornly hard to find, she notes, and it may be that "the reason we are seeing so much treatment-resistant asthma now, and so many allergies in the first place, is epigenetic; that is, a change in level of gene expression that could, in theory, be passed from parents to children to grandchildren."
Or, Garcia-Lloret continues, "Perhaps changes in levels of expression in respiratory genes that took place two generations ago are only showing up now" in fetuses of, say, African Americans born to mothers living in some of L.A.'s most severe smog 50 years ago. Add that to changes in diet, such as the steady rise of cheap sugary and fatty foods, and the rise in all kinds of inflammatory particles from wood smoke to uncontrolled stands of weeds on the city's periphery, and you have a kind of perfect respiratory storm.
In other words, as Garcia-Lloret says, "Between what you eat and what you breathe, you're screwed."
Tracking and Treating
Peter is lying down. He is always lying down, even early in the day. On this day he is attending the Breathmobile clinic with his mother, April, out on the Hudson playground, where the sounds of basketball and freeway mingle. The sound is a bit of a taunt to Peter: He would like to play sports when his breathing is normal, but even then, he cannot: He has severe joint pain.
"That's because of the side effects from medications," says Dr. Raffi Tachdjian '92, assistant professor of allergy and immunology at the David Geffen School of Medicine at UCLA, who is tending to Peter. "Here is a young person on six medications a day already. They do not work well. Here is a young person who wants to play sports, wants what everyone else wants, but he can't."
To help him cope, Tachdjian and the Breathmobile staff have put together a profile of Peter's "respiratory day" and the various asthma triggers throughout. When he is walking to school, he might have an exercise-induced fit that calls for one kind of med. Later in the day, when he is out on the playground, he may get an attack caused by pollen in the air. Or by high air temperature. Or, of course, by the high levels of traffic emissions wafting in from the freeway.
Knowing one's own warning signals makes a huge difference, but for patients with Peter's form of asthma most scientists look to a new generation of drugs informed by genetics. Tachdjian himself is studying one key genetic mutation. Dubbed Q576R, the gene has been associated with severe asthma in African Americans; 70 percent of that ethnic group carries the mutation, compared to 20 percent of the general population. Yet the causal relationship was unproven until research by Tachdjian and his colleagues found that the Q576R mutation was directly connected to an overactive Interleukin4 pathway — a firehouse gene that sounds the alarm for a huge spray of damaging molecules. The connection was so robust, Tachdjian wrote in the Journal of Experimental Medicine, "that novel therapeutic interventions may be beneficial to asthma treatment in this and other ethnic groups."
Eat Your Vegetables and Breathe Better
Those "novel therapeutic interventions" are already under serious study by Dr. Riedl, associate professor of medicine and section head of clinical immunology and allergy at UCLA. He became interested in the subject when he moved from Kansas City to Los Angeles for a postdoctoral internship.
"L.A. is hugely different from where I spent the first part of my life," he says. "I had friends telling me all about the freeways, about what was happening at schools next to freeways, and that made me hugely aware of the problem."
Riedl had a longstanding interest in respiratory disease and, like Nel, was interested in dietary treatments that increase our antioxidant levels, which could theoretically staunch the lung and heart damage from UFPs. But dietary antioxidant supplements — capsules and such — have largely turned out to be a bust, despite the incessant claims to the contrary by the ever-enterprising carnival barkers of modern nutrition.
Yet actual foods — greens, peppers, fruits, etc. — turn out to be good sources of active antioxidants; the problem is getting enough of them in your body to make a difference. For a few years, Riedl had been following experiments using concentrated broccoli sprouts at Johns Hopkins University and their effect on key internal antioxidants. Those internal free-radical fighters are controlled by a gene dubbed NrF2 transcription factor. The Johns Hopkins work also suggested the next step in making an anti-smog compound: Might some form of super-concentrated broccoli sprouts cause the body to make more of such protective molecules without side effects?
To find out, Riedl gave 65 adult human subjects increasing doses of a concentrated broccoli sprout compound. He introduced the compound in each subject's mouth. He then measured the expression of Phase II antioxidant enzymes, mediated by NrF2. What he found, he wrote, was that at each stage, ranging from zero to 200 grams, the antioxidant enzyme levels increased by consistent increments. In other words, its effects could be controlled like any pharmaceutical. There were almost no side effects.
Those results have pushed forward more research on broccoli sprout molecules. The end result, if all goes well, could be a pill or a nasal spray for children like Peter. In fact, it "could be the Holy Grail for us," says Riedl. "If we could somehow identify the subgroups of people who are deficient in Phase II antioxidants, you could essentially do a kind of targeted chemotherapy for environmental insults like UFPs."
The challenge is right in the wheelhouse of Dr. David Heber '69, Ph.D. '78, founding director of the UCLA Center for Human Nutrition and a professor of medicine and public health at the university, who is intensely focused on using the power of nutrition to make the human body more resistant to disease. Heber's research has helped move a number of research compounds — most notably red yeast rice for cholesterol control — out of the lab and onto store shelves. When he saw Nel's photo of a UFP entering a cell's mitochondria, he agreed to test the compound for its impact on the immune system.
The experiment itself — counting white blood cells in patients who breathe diesel particles and then take broccoli sprouts concentrate — is ongoing. Because Heber has submitted the experiment for review by the FDA, the endeavor has been laborious ("Every time we had them blow their nose, we had to call the FDA," he says), but its consequence could be huge.
"Nutrition may play a huge role in targeting these disease processes early on," contends Heber. "It is a great opportunity."
Peter and his mother are waiting.