During discussions of the Affordable Care Act, there was concern that some procedures would be harder to obtain. There was even worry about 'death panels' such as in the United Kingdom National Health Service.
It will be just the opposite in the short term, based on how utilization changed after earlier insurance reform in Massachusetts, according to an article by Chandy Ellimoottil, M.D., of the University of Michigan, Ann Arbor, and colleagues.
By looking at insurance expansion and utilization of discretionary and non-discretionary surgical procedures in one state, they project that surgery will go up - at least until taxpayers start getting the bill.
The authors used state inpatient databases from Massachusetts and two control states (New Jersey and New York) to identify adults who underwent discretionary procedures (e.g. elective procedures such as joint replacement and back surgery) and non-discretionary procedures (e.g. cancer surgery and hip fracture repair) from 2003 through 2010. The transition point for insurance reform was July 2007.
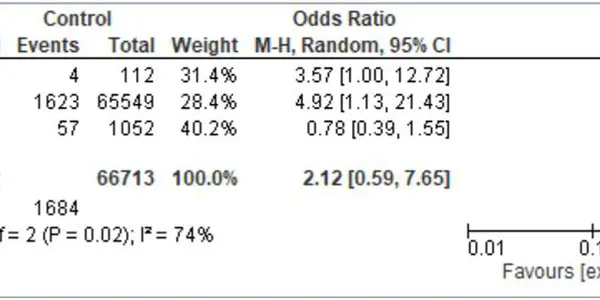
A total of 836,311 surgical procedures were identified during the study period. Insurance expansion was associated with a 9.3 percent increase in discretionary surgery in Massachusetts and a 4.5 percent decrease in nondiscretionary surgery. Authors estimate the ACA could yield an additional 465,934 discretionary surgical procedures by 2017.
"Our collective findings suggest that insurance expansion leads to greater utilization of discretionary inpatient procedures that are often performed to improve quality of life rather than to address immediately life-threatening conditions. Moving forward, research in this area should focus on whether greater utilization of such procedures represents a response to unmet need or changes in treatment thresholds driven by patients, providers or some combination of the two," they write.